CASE
A 50 year old female presented to us in
emergency with complaints of episodes of seizures and headache for past few days . MRI brain done at a private
institution revealed large olfactory grove meningioma measuring approximately
10 x 12 centimeters in size. Tumor was successfully removed by Dr Vineet Saggar
after eight hours of marathon surgery
and patient was discharged after few days without any neurological deficit.
Pre
Operative MRI of the Patient showing
large tumour


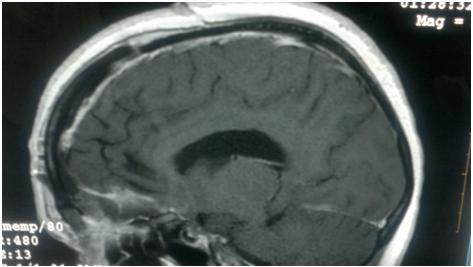
Post operative MRI showing complete
tumor removal

Meningiomas account for 15% of intracranial tumors and 90 percent of meningiomas are intracranial. They commonly occur in the fourth through sixth decades of life. They are more common in females and are rare in children
A meningioma
is a tumor of the meninges – membranes that line the skull and enclose the
brain. Meningiomas may arise from any location where meninges exist (eg, nasal
cavity, paranasal sinuses, middle ear, mediastinum) and are generally thought
to be slow-growing and benign. A meningioma can vary in size from a few
millimeters to many centimeters in diameter.
Olfactory groove meningiomas grow along the nerves that run
between the brain and the nose, the nerves allow you to smell. They can become
large without causing significant neurologic deficits or evidence of increased
intracranial pressure. Loss of smell can often be the only symptom. Changes in
mental status are seldom striking until the tumor has reached a large size.
Once the tumor becomes large it impinges on the optic nerves and chiasm
resulting in visual loss.

Olfactory groove meningioma. (A)
Incision and bone flap used for bifrontal craniootomy. (B) The
mucosa of the frontal sinus has been removed, and the sinus is packed with
bacitracin-soaked getfoam and covered with a flap of peiicranial tissue sewn to
the dura. (C) The anterior sagittal sinus is ligated. (D) The
blood supply coming in through the midline base of the skull is being occluded
and an internal decompression of the tumor done. (E) The capsule of the
tumor is being reflected into the area of internal tumor decompression and the
attachments to the surrounding brain divided. Minimal retraction is placed on
the surrounding brain. The major trunk of the anterior cerebral artery is
dissected off the tumor (arrow) but a branch going into the capsule is
coagulated and divided. (F) The posterior inferior capsule is dissected
off the arachnoid over the region of the optic nerve and internal carotid
artery (arrows). (G) The dural attachment has been excised. The bone
usually does not need to be removed. The area is covered with a graft of
perieranial tissue and gelfoam. MRI clearly defines the extent of the tumor,
the edema in the surrounding brain, the relationship of the optic nerves and
anterior cerebral arteries, and any extension into the ethmoid sinus . Angiography
is rarely needed. In our experience, there has been no indication for
preoperative embolization.
The indications for surgical treatment have been the presence of
neurological symptoms, which may include a change in mental function, headache,
disturbance in vision, or a seizure disorder, an asymptomatic patient with
edema in the adjacent brain areas, or MRI findings that the meningioma is near
the optic nerves. Radiation therapy is not recommended as a primary treatment
and would be used only to treat recurrence following radical subtotal removal.
Rarely does the patient report loss of sense of smell as a symptom,
although it is usually documented on examination. However, if olfaction is
still present the patient should be warned about the loss of this function,
since acute loss may be quite bothersome.
For patients with large tumors, we prefer a bifrontal craniotomy. . This
approach is associated with the smallest amount of retraction on the frontal
lobes, gives direct access to all sides of the tumor, and allows one to
decompress the tumor while working along the base of the skull to interrupt the
blood supply. For smaller tumors, a right subfrontal approach coming laterally
over the orbital roof may be used.
The key
considerations in the operation include:
1.
Dividing the attachments along
the skull base to interrupt the blood supply
2.
Doing an extensive internal decompression
of the tumor.
3.
Retracting the tumor capsule into
the area of decompression to keep traction on the frontal lobes to a minimum.
4.
Carefully separating the tumor
from attachments to the optic nerves and anterior cerebral arteries. The major
branches of the anterior cerebral arteries are usually separated from the tumor
by a rim of cerebral tissue or arachnoid but in large meningiomas these
arteries can be involved with the tumor capsule. Frontopolar and small branches
of the anterior cerebral arteries may be adherent to the posterior or superior
tumor capsule and can be taken with the tumor .
5.
Excising the dural attachment and
when present the hyperostotic bone, with care taken to avoid entering the
ethmoid sinus unless it is known that tumor extends into that area.
Covering the region
of the dural attachment with a graft of pericranial tissue and gelfoam.
Dr. Vineet Saggar (MCh)
Neuro Surgeon / Spinal Surgeon
Chandigarh, Mohali -
Ivy Hospital Sector 71
+91-9855990990
http://www.neurosurgeoninchandigarh.com
http://neurosurgeonhead.blogspot.in/
http://www.facebook.com/neuro.surgeon.7186
http://www.slideshare.net/neurosergeonheadNeuro Surgeon / Spinal Surgeon
Chandigarh, Mohali -
Ivy Hospital Sector 71
+91-9855990990
http://www.neurosurgeoninchandigarh.com
http://neurosurgeonhead.blogspot.in/
http://www.facebook.com/neuro.surgeon.7186
No comments:
Post a Comment